Entry
Reader's guide
Entries A-Z
Subject index
Brain and Trauma
Psychological trauma can have lasting effects on the brain. These effects underlie symptoms of posttrau-matic stress disorder (PTSD), as well as depression, substance abuse, dissociative disorders, and borderline personality disorder (BPD). Brain areas affected by trauma that also mediate the stress response include the amygdala, hippocampus, and medial prefrontal cortex (including the anterior cingulate).
Trauma spectrum psychiatric disorders represent the behavioral manifestation of stress-induced changes in brain structure and function. Stress results in acute and chronic changes in neurochemical systems and specific brain regions, which result in long-term changes in brain “circuits” involved in the stress response.
Hormones (including norepinephrine and cortisol) play a critical role in the stress response. However, chronic stress can lead to dysfunction of these systems. Norepinephrine (adrenaline) is released in both the brain and the body, and has several functions that are critical for survival. Norepinephrine sharpens the senses, focuses attention, raises the level of fear, quickens the heart rate and blood pressure, and in general prepares us for the worst. The norepinephrine system is like a fire alarm that alerts all areas of the brain simultaneously. This system sacrifices the ability to convey specific information to specific parts of the brain in order to obtain more speed. Norepinephrine focuses the senses by activating the neurons that collect information, preparing the body for fight or flight. At the same time, it stimulates the heart to beat more rapidly and blood pressure to increase, causing a rapid transfer of oxygen and nutrients needed for survival to all the cells of the body. Chronic stress in animals leads to increased levels of norepinephrine.
PTSD is associated with long-term dysregulation of the noradrenergic system. Psychophysiology studies have demonstrated an increase in sympathetic nervous system responses (e.g., heart rate, blood pressure, and galvanic skin response) to traumatic reminders. Other studies showed increased nor-epinephrine in plasma and urine at baseline and in response to traumatic reminders. Administration of the alpha2 antagonist yohimbine, which causes an increased release of norepinephrine in the brain, resulted in an increase in PTSD-specific symptomatology, as well as greater release of norepinephrine metabolites in plasma, in PTSD patients. Alterations in brain responses to stimulation of the norepinephrine system with yohimbine were also found in PTSD patients as measured with positron emission tomography (PET).
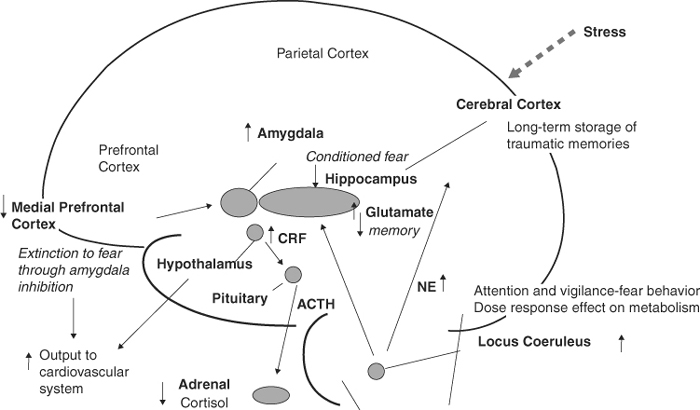
Figure 1 Impact of Trauma on the Brain. Trauma has lasting effects on the brain, including norepinephrine and cortisol systems and brain areas including the hippocampus, amygdala, and medial prefrontal cortex (mPFC).
The cortisol system also plays an important role in the stress response. Cortisol redistributes energy to enhance survival, suppressing functions not needed for immediate survival, such as reproduction, the body's immune response, digestion, and the feeling of pain, and shunting energy to the brain and muscles. Although useful in the short run, this may occur at the expense of long-term viability of the body. With chronic cortisol elevation, there is increased risk of gastric ulcers, thinning of the bones, cognitive dysfunction, and other problems.
The corticotropin-releasing factor (CRF) is released in the brain during stress, and causes release of adrenocorticotropin-releasing hormone (ACTH) from the pituitary, which in turn stimulates release of cortisol from the adrenal gland. Stress can result in long-term increases in CRF-potentiated release of cortisol with subsequent stressors. PTSD has been associated with long-term dysregulation of the hypothalamic-pituitary-adrenal (HPA) axis. Baseline levels of urinary cortisol were either decreased or unchanged in chronic PTSD, but decreased levels were found in 24-hour samples of plasma cortisol levels, and stressors or traumatic reminders are associated with potentiated release of cortisol. PTSD was associated with a super-suppression of the cortisol response to lower doses of the synthetic form of cortisol, dexamethasone (0.5 mg), a finding that is the opposite of patients with major depression who are nonsuppressors with the standard 1 mg DST test. PTSD patients also had elevated levels of CRF in the cerebrospinal fluid.
...
- Anthropology and Archaeology
- Anthropology and Trauma
- Anthropology and War
- Racial and Ethnic Factors
- Racial Variations in the Psychobiology of Trauma
- Resource Loss Among Adults, Groups, and Communities
- Resource Loss Among Children and Families
- Rituals and Ceremonies, Therapeutic Use of
- Role of Trauma in Ethnic and Cultural Identity
- War, Origins in Animals and Early Societies
- Wars for Symbols
- Wars in Civilized Societies
- Arts and Humanities
- Business and Economics
- Children and Families
- Abduction/Kidnapping
- African Women and Girls' Trauma
- Campus Violence
- Childhood and Adolescent Trauma: An Overview
- Childhood and Adolescent Trauma: Assessment and Treatment
- Childhood Trauma and the Juvenile Justice System
- Childhood Traumatic Stress
- Children of War
- Critical Illness in Children
- Dissociative Identity Disorder and Trauma
- Family and Couples Trauma and Treatment
- Family-Based Treatment for Child Traumatic Stress
- Genetic Epidemiology
- Incest
- Marital Rape
- Marriage and the Marital Relationship
- Military Families, Effects of Combat and Deployment on
- Parenting During and After Traumatic Events
- Perinatal Trauma
- Perinatal Trauma, Long-Term Consequences of
- Protective Factors in Childhood Posttraumatic Stress Disorder
- Resilient Posttraumatic Adjustment in Childhood and Beyond
- Resource Loss Among Adults, Groups, and Communities
- Resource Loss Among Children and Families
- School Shootings
- Systemic Trauma Research
- Transgenerational Transmission of Trauma
- Crime and Law
- Abduction/Kidnapping
- Battered Women
- Blaming the Victim
- Campus Violence
- Childhood Trauma and the Juvenile Justice System
- Clergy, Sexual Abuse by
- Community Violence
- Comstock Act
- Correctional Officers and Trauma
- Crime Scene Investigation
- Criminal Behavior Consequent to War
- Date Rape/Acquaintance Rape
- Genocide
- Genocide in Non-Western Nations
- Genocide, Cambodia's Mass Casualty Trauma
- Hate Crimes
- Homicide and Trauma
- Human Trafficking
- Incarceration and Trauma
- Incest
- Law Enforcement Officers
- Lawsuits Against Behavioral Health Professionals
- Lawsuits Against Medical Professionals
- Male Rape
- Marital Rape
- Mass Violence
- Military Sexual Abuse
- Murder
- Perpetrators of Trauma
- Psychological Injury and Law
- Rapist Profiles
- School Shootings
- Secondary Trauma Among First Responders
- Secondary Trauma Among Judges, Jurors, Attorneys, and Courtroom Personnel
- Sexual Assault and Trauma
- Sexual Assault, Drug Facilitated
- Sexual Compulsion and Trauma
- Sexual Harassment of Women
- Sexual Predators
- Sexual Trauma, Causes of
- Slavery and Forced Servitude
- Social Learning Theory and Sexual Aggression
- Survival and Coping After Rape
- Terrorism, History of
- Trauma and Domestic Violence
- Wartime Rape
- Workplace Violence
- Crisis and Disaster
- Community Disasters
- Critical Incident Stress
- Debriefing
- Disaster Medicine
- Disaster Mortuary Services
- Disaster-Related Trauma
- Disasters, History of
- Early Interventions
- Emergency Care and Services
- First Responders and Trauma
- Humanitarian Missions
- Peacekeeping Missions
- Psychobiology of Crisis
- Psychological First Aid
- Psychological First Aid for Older Adults
- Psychospiritual Impact of Disaster
- Resilience and Hurricane Katrina
- Role of Media in Managing Disasters
- Culture and Ethnicity
- African American Culture and Trauma
- African Women and Girls' Trauma
- Cultural Aspects of Trauma
- Cultural Diversity in Trauma Response
- Culture and Cultural Beliefs
- Culture and Trauma
- Ethnicity, Culture, and Disaster Response
- Genocide
- Genocide in Non-Western Nations
- Genocide, Cambodia's Mass Casualty Trauma
- Nongovernmental Organizations, Governments, and Humanitarian Aid
- Race-Based Traumatic Stress
- Racial and Ethnic Factors
- Racial Variations in the Psychobiology of Trauma
- Racism-Induced Trauma
- Refugees
- Rituals and Ceremonies, Therapeutic Use of
- Role of Trauma in Ethnic and Cultural Identity
- Slavery and Forced Servitude
- Traumatization in the Name of Religion
- Death and Dying
- Ethics and Philosophy
- Assisted Suicide
- Boundaries and Boundary Violations
- Boundary Issues for Traumatologists
- Counterbalancing Stress
- Countertransference
- Ethical Dilemmas in Treatment of Trauma
- Ethics
- Humor and Trauma
- Philosophy and Ethics of Trauma Treatments
- Philosophy of Trauma
- Philosophy of Trauma Nursing
- Secondary Trauma Among Behavioral Health Professionals
- Secondary Trauma Among Chaplains
- Secondary Trauma Among First Responders
- Secondary Trauma Among Judges, Jurors, Attorneys, and Courtroom Personnel
- Secondary Trauma Among Medical Professionals
- Secondary Trauma Among Medics and Corpsmen
- Secondary Traumatic Stress
- Shame
- Trauma Caregivers
- Trauma Memories: Research and Ethics
- First Responders
- History
- Humanitarian Aid
- Internet, the Media, and Entertainment
- Medicine
- Abortion
- Alcohol and Trauma
- Assisted Suicide
- Brain and Trauma
- Combat Medics and Corpsmen
- Critical Illness in Children
- Disaster Medicine
- Lawsuits Against Medical Professionals
- Medical Marijuana and Posttraumatic Stress Disorder
- Medical Trauma Research
- Pain
- Perinatal Trauma
- Perinatal Trauma, Long-Term Consequences of
- Pharmacotherapy
- Philosophy of Trauma Nursing
- Primary Care
- Psychopharmacology, Psychiatry, and Trauma
- Public Health
- Retraumatization
- Secondary Trauma Among Medical Professionals
- Sexual Assault, Drug Facilitated
- Somatic Complaints
- Trauma-Related Physical Symptoms and Illnesses
- Traumatized Nurses
- Traumatized Physicians
- Natural Sciences
- Biological Effects of Physical and Psychological Trauma
- Biological Mechanism of Traumatic Stress Response
- Biology and Posttraumatic Stress Disorder
- Brain and Memory
- Brain and Trauma
- Encoding Trauma, Neurobiology of
- Genetic Epidemiology
- Hippocampus
- Limbic System
- Neurobiological Effects of Trauma
- Neurobiology of Posttraumatic Stress Disorder and Suicide
- Psychobiology of Crisis
- Trauma and Metabolic Syndrome
- Trauma Resilience, Ecology of
- Traumatic Inventions and the Ethics of Scientific Discovery
- Traumatized Scientists
- Psychology and Psychiatry
- Acute Stress Disorder
- Biological Mechanism of Traumatic Stress Response
- Brain and Memory
- Burnout
- Clinical Trauma Psychology
- Cognitive Behavioral Therapy
- Cognitive Processing Therapy
- Cognitive Restructuring and Trauma
- Combat Stress Control
- Combat-Related Posttraumatic Stress Disorder
- Compassion Fatigue
- Complex Trauma
- Conservation of Resources Theory
- Counseling and Education About Trauma
- Counterbalancing Stress
- Countertransference
- Dissociation
- Dissociative Identity Disorder and Trauma
- Evidence-Based Practice
- Eye Movement Desensitization and Reprocessing: Theory and Research
- Eye Movement Desensitization and Reprocessing: Treatment
- Family and Couples Trauma and Treatment
- Family-Based Treatment for Child Traumatic Stress
- Fragility, Posttraumatic
- Iatrogenic Effects
- Lawsuits Against Behavioral Health Professionals
- Limbic System
- Marriage and the Marital Relationship
- Meditation
- Memory Work
- Military Psychology and Combat Stress Injuries
- Mowrer's Two-Factor Theory
- Pain
- Personality Disorders
- Pharmacotherapy
- Posttraumatic Stress Disorder
- Posttraumatic Stress Disorder Assessment and Systemic Treatment
- Posttraumatic Stress Disorder, Comorbidity
- Primary Care
- Promoting Resilience in the Traumatized
- Protective Factors in Childhood Posttraumatic Stress Disorder
- Psychological Injury and Law
- Psychological Responses to Trauma
- Psychological Trauma
- Psychological Trauma Research
- Psychoneuroimmunology and Trauma
- Psychopharmacology, Psychiatry, and Trauma
- Psychosensory Therapy
- Rape Counseling
- Rape Crisis Centers
- Rape Trauma Syndrome
- Recovery From Trauma
- Relapse Prevention and Posttraumatic Stress Disorder
- Resilience
- Resilience Bolstering
- Resilience, Growth, and Thriving
- Retraumatization
- Secondary Trauma Among Behavioral Health Professionals
- Secondary Traumatic Stress
- Shame
- Social Learning Theory and Sexual Aggression
- Social Support and Trauma
- Somatic Complaints
- Stigma
- Stress Inoculation Training
- Suicide
- Survival and Coping After Rape
- Systemic Trauma Research
- Theories of Psychological Stress
- Trauma and Selfhood
- Trauma and Sexuality
- Trauma Assessment
- Trauma Education
- Trauma Prevention
- Trauma Psychology Research
- Trauma Triggers
- Trauma-Related Happiness and Pleasure
- Trauma-Related Physical Symptoms and Illnesses
- Trauma, Causes of
- Trauma, Identity, and the Workplace
- Traumatic Stress and Resilience
- Traumatic Stress Responses
- Traumatized Practitioners, Supervisors of
- Victim, Survivor, Thriver
- Virtual Reality Exposure Therapy
- Vulnerability, Posttraumatic
- Public Health
- Religion and Spirituality
- Clergy, Counseling by
- Clergy, Sexual Abuse by
- Combat Chaplains
- Cults and Sects
- Growth, Posttraumatic
- Meditation
- Posttraumatic Growth Among Asylum Seekers and Other Immigrants
- Psychospiritual Impact of Disaster
- Religious and Pastoral Responses to Trauma
- Religious Fundamentalism
- Secondary Trauma Among Chaplains
- Spiritual and Religious Growth
- Spiritual Intelligence and Posttraumatic Growth
- Traumatization in the Name of Religion
- Social Work
- Battered Women
- Bereavement
- Cognitive Behavioral Therapy
- Cognitive Processing Therapy
- Comstock Act
- Ethics
- Evidence-Based Practice
- Military Social Work and Combat Stress Management
- Social Support and Trauma
- Social Work With the Traumatized Homeless
- Theories of Psychological Stress
- Trauma and Domestic Violence
- Trauma and Homelessness
- Trauma and Social Work Practice
- Trauma Research, Social Work Contributions to
- Traumatized Practitioners, Supervisors of
- Sociology
- Traumatology and Trauma Recovery
- Acute Stress Disorder
- Additive Trauma
- Alcohol and Trauma
- Bearing Witness to Trauma
- Biology and Posttraumatic Stress Disorder
- Clergy, Counseling by
- Clinical Trauma Psychology
- Cognitive Restructuring and Trauma
- Compassion Fatigue
- Complex Trauma
- Conspiracy of Silence
- Counseling and Education About Trauma
- Cultural Aspects of Trauma
- Cultural Diversity in Trauma Response
- Culture and Trauma
- Cumulative Trauma
- Dance and Trauma
- Despair, Posttraumatic
- Disaster-Related Trauma
- Early Interventions
- Encoding Trauma, Neurobiology of
- Ethical Dilemmas in Treatment of Trauma
- Eye Movement Desensitization and Reprocessing: Theory and Research
- Eye Movement Desensitization and Reprocessing: Treatment
- Fear, Posttraumatic
- Fragility, Posttraumatic
- Grief and Mourning
- Grief, Complicated
- Growth, Posttraumatic
- Hippocampus
- Homicide and Trauma
- Humor and Trauma
- Hypnosis in the Treatment of Posttraumatic Stress Disorder
- Iatrogenic Effects
- Incarceration and Trauma
- Literary Expressions of Trauma
- Managing Trauma Symptoms
- Medical Marijuana and Posttraumatic Stress Disorder
- Medical Trauma Research
- Military Trauma
- Neurobiological Effects of Trauma
- Neurobiology of Posttraumatic Stress Disorder and Suicide
- Perpetrators of Trauma
- Philosophy and Ethics of Trauma Treatments
- Philosophy of Trauma
- Poetry and Trauma
- Posttraumatic Growth Among Asylum Seekers and Other Immigrants
- Posttraumatic Stress Disorder
- Posttraumatic Stress Disorder Assessment and Systemic Treatment
- Posttraumatic Stress Disorder, Comorbidity
- Posttraumatic Stress Disorder, History of
- Prolonged Exposure
- Promoting Resilience in the Traumatized
- Psychological Responses to Trauma
- Psychological Trauma
- Psychological Trauma Research
- Psychoneuroimmunology and Trauma
- Psychosensory Therapy
- Rape Counseling
- Rape Crisis Centers
- Rape Trauma Syndrome
- Rapist Profiles
- Recovery From Trauma
- Relapse Prevention and Posttraumatic Stress Disorder
- Resilience
- Resilience and Hurricane Katrina
- Resilience Bolstering
- Resilience, Growth, and Thriving
- Sanctuary Model
- Self-Regulation
- Sexual Compulsion and Trauma
- Sexual Harassment of Women
- Sexual Predators
- Sexual Trauma, Causes of
- Shared Trauma
- Silencing Response
- Stigma
- Suicide
- Transgenerational Transmission of Trauma
- Trauma and Autobiography
- Trauma and Homelessness
- Trauma and Metabolic Syndrome
- Trauma and Metaphor
- Trauma and Selfhood
- Trauma and Sexuality
- Trauma and Social Work Practice
- Trauma as Entertainment
- Trauma Assessment
- Trauma Caregivers
- Trauma Education
- Trauma Memories: Research and Ethics
- Trauma Prevention
- Trauma Psychology Research
- Trauma Survival Strategies
- Trauma Triggers
- Trauma-Organized Systems
- Trauma-Related Happiness and Pleasure
- Trauma, Causes of
- Trauma, Definitions of
- Traumatic Bereavement
- Traumatic Stress and Resilience
- Traumatic Stress Responses
- Traumatized Scientists
- Traumatology
- Vicarious Trauma
- Victim, Survivor, Thriver
- Virtual Reality Exposure Therapy
- Vulnerability, Posttraumatic
- War Crimes
- War and Combat
- Anthropology and War
- Children of War
- Combat Chaplains
- Combat Medics and Corpsmen
- Combat Mortuary Services
- Combat Stress Control
- Combat-Related Posttraumatic Stress Disorder
- Combat-Related Stress Injury: Theory, Research, and Management
- Criminal Behavior Consequent to War
- Death Notification in War
- Military Families, Effects of Combat and Deployment on
- Military Psychology and Combat Stress Injuries
- Military Sexual Abuse
- Military Social Work and Combat Stress Management
- Military Trauma
- Secondary Trauma Among Medics and Corpsmen
- War Crimes
- War, Origins in Animals and Early Societies
- Wars for Symbols
- Wars in Civilized Societies
- Wartime Rape
- Loading...
Get a 30 day FREE TRIAL
-
 Watch videos from a variety of sources bringing classroom topics to life
Watch videos from a variety of sources bringing classroom topics to life -
Read modern, diverse business cases
-
Explore hundreds of books and reference titles

Read next

More like this
Sage Recommends
We found other relevant content for you on other Sage platforms.
Have you created a personal profile? Login or create a profile so that you can save clips, playlists and searches