Entry
Reader's guide
Entries A-Z
Subject index
Cardiovascular Disease
Cardiovascular disease (CVD) ranks as the leading cause of morbidity and mortality among developed countries and is rapidly emerging as the predominant cause of death in many developing countries. There are numerous differences in incidence across ethnic groups and geographic regions within countries. Coronary heart disease (CHD) is the predominant manifestation of CVD and responsible for the majority of cases of CVD in developed countries. Numerous longitudinal epidemiological studies conducted in the past 60 years have provided valuable insight into the natural history and risk factors associated with the development of and prognosis associated with CVD. Randomized clinical trials have demonstrated the value of treatment of several key risk factors, most notably hypertension and hypercholesterolemia, for both the primary and the secondary prevention of CVD. This entry reviews the descriptive epidemiology of CVD, its associated risk factors, assessment of CVD risk, and the evidence behind the control of CVD risk factors for the prevention of CVD.
Definitions, Incidence, and Distribution
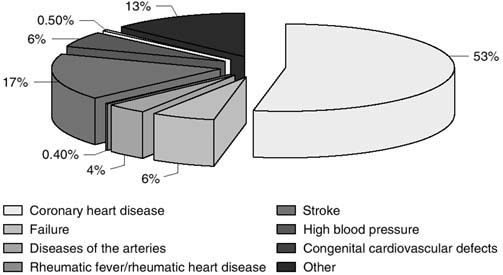
CVD comprises many conditions, including CHD, heart failure, rheumatic fever or rheumatic heart disease, stroke, and congenital heart disease. Of these, 7 in 10 deaths from CVD are due to CHD (53%) and stroke (17%) (Figure 1). CHD, the most common CVD condition, increases in prevalence directly with age in both men and women (Figure 2).
Myocardial infarction, angina pectoris (especially if requiring hospitalization), and sudden coronary death are the major clinical manifestations of CHD. CHD initially presents as sudden coronary death in approximately one third of the cases. Other forms of documented CHD include procedures done as a result of documented significant atherosclerosis, such as coronary artery bypass grafting (CABG) or percutaneous coronary interventions (PCI), including angioplasty and stenting. Persons with documented significant disease from a coronary angiogram, echocardiogram, nuclear myocardial perfusion, magnetic resonance imaging, or computed tomography angiographic or coronary calcium scan can also confirm the presence and extent of coronary artery disease; however, because the definitions used to define significant disease vary and/or such results do not typically result in hospitalization, these cases are not normally counted as incident or prevalent CHD, nor are they considered ‘hard’ (usually death or hospitalized diagnosed conditions) cardiovascular endpoints for the purposes of clinical trials. Nonfatal or fatal myocardial infarction and sudden coronary death are most typically included as ‘hard’ CHD endpoints.
Figure 1 Percentage Breakdown of Deaths From Cardiovascular Disease
Mortality rates from CVD and CHD vary widely across different countries. From the most recent data available, among men, CVD death rates per 100,000 range from 170 in Japan to 1,167 in the Russian Federation, with the United States at 307. Corresponding CHD death rates were 53, 639, and 187, respectively. Among women, these rates were lowest in France but highest in the Russian Federation, with intermediate rates in the United States. These rates were 69, 540, and 158 for CVD, respectively, and 18, 230, and 77 for CHD, respectively. Next to the Russian Federation, Romania, Bulgaria, and Hungary had the next highest rates both for CVD and CHD. Spain, Australia, Switzerland, and France (or Japan) were the other countries with the lowest rates.
...
- Behavioral and Social Science
- Acculturation
- Bioterrorism
- Community Health
- Community Trial
- Community-Based Participatory Research
- Cultural Sensitivity
- Demography
- Determinants of Health Model
- Ecological Fallacy
- Epidemiology in Developing Countries
- EuroQoL EQ-5D Questionnaire
- Functional Status
- Genocide
- Geographical and Social Influences on Health
- Health Behavior
- Health Belief Model
- Health Communication
- Health Communication in Developing Countries
- Health Disparities
- Health Literacy
- Health, Definitions of
- Life Course Approach
- Locus of Control
- Medical Anthropology
- Network Analysis
- Participatory Action Research
- Poverty and Health
- Quality of Life, Quantification of
- Quality of Well-Being Scale (QWB)
- Race and Ethnicity, Measurement Issues With
- Race Bridging
- Rural Health Issues
- Self-Efficacy
- SF-36® Health Survey
- Social Capital and Health
- Social Epidemiology
- Social Hierarchy and Health
- Social Marketing
- Social-Cognitive Theory
- Socioeconomic Classification
- Spirituality and Health
- Targeting and Tailoring
- Theory of Planned Behavior
- Transtheoretical Model
- Urban Health Issues
- Urban Sprawl
- Branches of Epidemiology
- Applied Epidemiology
- Chronic Disease Epidemiology
- Clinical Epidemiology
- Descriptive and Analytic Epidemiology
- Disability Epidemiology
- Disaster Epidemiology
- Eco-Epidemiology
- Environmental and Occupational Epidemiology
- Field Epidemiology
- Genetic Epidemiology
- Injury Epidemiology
- Maternal and Child Health Epidemiology
- Molecular Epidemiology
- Neuroepidemiology
- Nutritional Epidemiology
- Pharmacoepidemiology
- Psychiatric Epidemiology
- Reproductive Epidemiology
- Social Epidemiology
- Veterinary Epidemiology
- Diseases and Conditions
- Alzheimer's Disease
- Anxiety Disorders
- Arthritis
- Asthma
- Autism
- Avian Flu
- Bipolar Disorder
- Bloodborne Diseases
- Cancer
- Cardiovascular Disease
- Diabetes
- Foodborne Diseases
- Gulf War Syndrome
- Hepatitis
- HIV/AIDS
- Hypertension
- Influenza
- Insect-Borne Disease
- Malaria
- Measles
- Oral Health
- Osteoporosis
- Parasitic Diseases
- Plague
- Polio
- Post-Traumatic Stress Disorder
- Schizophrenia
- Severe Acute Respiratory Syndrome (SARS)
- Sexually Transmitted Diseases
- Sick Building Syndrome
- Sleep Disorders
- Smallpox
- Suicide
- Toxic Shock Syndrome
- Tuberculosis
- Vector-Borne Disease
- Vehicle-Related Injuries
- Vitamin Deficiency Diseases
- Waterborne Diseases
- Yellow Fever
- Zoonotic Disease
- Epidemiological Concepts
- Attack Rate
- Attributable Fractions
- Biomarkers
- Birth Cohort Analysis
- Birth Defects
- Case Definition
- Case Reports and Case Series
- Case-Cohort Studies
- Case-Fatality Rate
- Cohort Effects
- Community Trial
- Competencies in Applied Epidemiology for Public Health Agencies
- Cumulative Incidence
- Direct Standardization
- Disease Eradication
- Effect Modification and Interaction
- Effectiveness
- Efficacy
- Emerging Infections
- Epidemic
- Etiology of Disease
- Exposure Assessment
- Fertility, Measures of
- Fetal Death, Measures of
- Gestational Age
- Health, Definitions of
- Herd Immunity
- Hill's Considerations for Causal Inference
- Incidence
- Indirect Standardization
- Koch's Postulates
- Life Course Approach
- Life Expectancy
- Life Tables
- Malnutrition, Measurement of
- Mediating Variable
- Migrant Studies
- Mortality Rates
- Natural Experiment
- Notifiable Disease
- Outbreak Investigation
- Population Pyramid
- Preclinical Phase of Disease
- Preterm Birth
- Prevalence
- Prevention: Primary, Secondary, and Tertiary
- Public Health Surveillance
- Qualitative Methods in Epidemiology
- Quarantine and Isolation
- Screening
- Sensitivity and Specificity
- Sentinel Health Event
- Syndemics
- Epidemiologic Data
- Administrative Data
- American Cancer Society Cohort Studies
- Behavioral Risk Factor Surveillance System
- Biomedical Informatics
- Birth Certificate
- Cancer Registries
- Death Certificate
- Framingham Heart Study
- Global Burden of Disease Project
- Harvard Six Cities Study
- Health Plan Employer Data and Information Set
- Healthcare Cost and Utilization Project
- Healthy People 2010
- Honolulu Heart Program
- Illicit Drug Use, Acquiring Information on
- Medical Expenditure Panel Survey
- Monitoring the Future Survey
- National Ambulatory Medical Care Survey
- National Death Index
- National Health and Nutrition Examination Survey
- National Health Care Survey
- National Health Interview Survey
- National Immunization Survey
- National Maternal and Infant Health Survey
- National Mortality Followback Survey
- National Survey of Family Growth
- Physicians' Health Study
- Pregnancy Risk Assessment and Monitoring System
- Relational Database
- Rochester Epidemiology Project
- Sampling Techniques
- Secondary Data
- Spreadsheet
- Youth Risk Behavior Surveillance System
- Ethics
- Genetics
- Association, Genetic
- Chromosome
- Epigenetics
- Family Studies in Genetics
- Gene
- Gene-Environment Interaction
- Genetic Counseling
- Genetic Disorders
- Genetic Epidemiology
- Genetic Markers
- Genomics
- Genotype
- Hardy-Weinberg Law
- Heritability
- Human Genome Project
- Icelandic Genetics Database
- Linkage Analysis
- Molecular Epidemiology
- Multifactorial Inheritance
- Mutation
- Newborn Screening Programs
- Phenotype
- Teratogen
- Twin Studies
- Health Care Economics and Management
- Biomedical Informatics
- EuroQoL EQ-5D Questionnaire
- Evidence-Based Medicine
- Formulary, Drug
- Functional Status
- Health Care Delivery
- Health Care Services Utilization
- Health Economics
- International Classification of Diseases
- International Classification of Functioning, Disability, and Health
- Managed Care
- Medicaid
- Medicare
- Partner Notification
- Quality of Life, Quantification of
- Quality of Well-Being Scale (QWB)
- SF-36® Health Survey
- Health Risks and Health Behaviors
- Agent Orange
- Alcohol Use
- Allergen
- Asbestos
- Bioterrorism
- Child Abuse
- Cholesterol
- Circumcision, Male
- Diabetes
- Drug Abuse and Dependence, Epidemiology of
- Eating Disorders
- Emerging Infections
- Firearms
- Foodborne Diseases
- Harm Reduction
- Hormone Replacement Therapy
- Intimate Partner Violence
- Lead
- Love Canal
- Malnutrition, Measurement of
- Mercury
- Obesity
- Oral Contraceptives
- Pain
- Physical Activity and Health
- Pollution
- Poverty and Health
- Radiation
- Sexual Risk Behavior
- Sick Building Syndrome
- Social Capital and Health
- Social Hierarchy and Health
- Socioeconomic Classification
- Spirituality and Health
- Stress
- Teratogen
- Thalidomide
- Tobacco
- Urban Health Issues
- Urban Sprawl
- Vehicle-Related Injuries
- Violence as a Public Health Issue
- Vitamin Deficiency Diseases
- War
- Waterborne Diseases
- Zoonotic Disease
- History and Biography
- Budd, William
- Doll, Richard
- Ehrlich, Paul
- Epidemiology, History of
- Eugenics
- Farr, William
- Frost, Wade Hampton
- Genocide
- Goldberger, Joseph
- Graunt, John
- Hamilton, Alice
- Hill, Austin Bradford
- Jenner, Edward
- Keys, Ancel
- Koch, Robert
- Lind, James
- Lister, Joseph
- Nightingale, Florence
- Pasteur, Louis
- Public Health, History of
- Reed, Walter
- Ricketts, Howard
- Rush, Benjamin
- Snow, John
- Tukey, John
- Tuskegee Study
- Infrastructure of Epidemiology and Public Health
- American College of Epidemiology
- American Public Health Association
- Association of Schools of Public Health
- Centers for Disease Control and Prevention
- Council of State and Territorial Epidemiologists
- European Public Health Alliance
- European Union Public Health Programs
- Food and Drug Administration
- Governmental Role in Public Health
- Healthy People 2010
- Institutional Review Board
- Journals, Epidemiological
- Journals, Public Health
- National Center for Health Statistics
- National Institutes of Health
- Pan American Health Organization
- Peer Review Process
- Public Health Agency of Canada
- Publication Bias
- Society for Epidemiologic Research
- Surgeon General, U.S.
- U.S. Public Health Service
- United Nations Children's Fund
- World Health Organization
- Medical Care and Research
- Allergen
- Apgar Score
- Barker Hypothesis
- Birth Defects
- Body Mass Index (BMI)
- Carcinogen
- Case Reports and Case Series
- Clinical Epidemiology
- Clinical Trials
- Community Health
- Community Trial
- Comorbidity
- Complementary and Alternative Medicine
- Effectiveness
- Efficacy
- Emerging Infections
- Etiology of Disease
- Evidence-Based Medicine
- Gestational Age
- Intent-to-Treat Analysis
- International Classification of Diseases
- International Classification of Functioning, Disability, and Health
- Latency and Incubation Periods
- Life Course Approach
- Malnutrition, Measurement of
- Medical Anthropology
- Organ Donation
- Pain
- Placebo Effect
- Preclinical Phase of Disease
- Preterm Birth
- Public Health Nursing
- Quarantine and Isolation
- Screening
- Vaccination
- Specific Populations
- African American Health Issues
- Aging, Epidemiology of
- American Indian Health Issues
- Asian American/Pacific Islander Health Issues
- Breastfeeding
- Child and Adolescent Health
- Epidemiology in Developing Countries
- Hormone Replacement Therapy
- Immigrant and Refugee Health Issues
- Latino Health Issues
- Maternal and Child Health Epidemiology
- Men's Health Issues
- Oral Contraceptives
- Race and Ethnicity, Measurement Issues With
- Race Bridging
- Rural Health Issues
- Sexual Minorities, Health Issues of
- Urban Health Issues
- Women's Health Issues
- Statistics and Research Methods
- F Test
- p Value
- Additive and Multiplicative Models
- Analysis of Covariance
- Analysis of Variance
- Bar Chart
- Bayes's Theorem
- Bayesian Approach to Statistics
- Bias
- Binomial Variable
- Birth Cohort Analysis
- Box-and-Whisker Plot
- Capture-Recapture Method
- Categorical Data, Analysis of
- Causal Diagrams
- Causation and Causal Inference
- Censored Data
- Central Limit Theorem
- Chi-Square Test
- Classification and Regression Tree Models
- Cluster Analysis
- Coefficient of Determination
- Cohort Effects
- Collinearity
- Community Trial
- Community-Based Participatory Research
- Confidence Interval
- Confounding
- Control Group
- Control Variable
- Convenience Sample
- Cox Model
- Critical Value
- Cumulative Incidence
- Data Management
- Data Transformations
- Decision Analysis
- Degrees of Freedom
- Dependent and Independent Variables
- Diffusion of Innovations
- Discriminant Analysis
- Dose-Response Relationship
- Doubling Time
- Dummy Coding
- Dummy Variable
- Ecological Fallacy
- Economic Evaluation
- Effect Modification and Interaction
- Factor Analysis
- Fisher's Exact Test
- Geographical and Spatial Analysis
- Graphical Presentation of Data
- Halo Effect
- Hawthorne Effect
- Hazard Rate
- Healthy Worker Effect
- Hill's Considerations for Causal Inference
- Histogram
- Hypothesis Testing
- Inferential and Descriptive Statistics
- Intent-to-Treat Analysis
- Internet Data Collection
- Interquartile Range
- Interrater Reliability
- Intervention Studies
- Interview Techniques
- Kaplan-Meier Method
- Kappa
- Kurtosis
- Latent Class Models
- Life Tables
- Likelihood Ratio
- Likert Scale
- Log-Rank Test
- Logistic Regression
- Longitudinal Research Design
- Matching
- Measurement
- Measures of Association
- Measures of Central Tendency
- Measures of Variability
- Meta-Analysis
- Missing Data Methods
- Multilevel Modeling
- Multiple Comparison Procedures
- Multivariate Analysis of Variance
- Natural Experiment
- Network Analysis
- Nonparametric Statistics
- Normal Distribution
- Null and Alternative Hypotheses
- Observational Studies
- Overmatching
- Panel Data
- Participatory Action Research
- Pearson Correlation Coefficient
- Percentiles
- Person-Time Units
- Pie Chart
- Placebo Effect
- Point Estimate
- Probability Sample
- Program Evaluation
- Propensity Score
- Proportion
- Qualitative Methods in Epidemiology
- Quasi Experiments
- Questionnaire Design
- Race Bridging
- Random Variable
- Random-Digit Dialing
- Randomization
- Rate
- Ratio
- Receiver Operating Characteristic (ROC) Curve
- Regression
- Relational Database
- Reliability
- Response Rate
- Robust Statistics
- Sample Size Calculations and Statistical Power
- Sampling Distribution
- Sampling Techniques
- Scatterplot
- Secondary Data
- Sensitivity and Specificity
- Sequential Analysis
- Simpson's Paradox
- Skewness
- Spreadsheet
- Stem-and-Leaf Plot
- Stratified Methods
- Structural Equation Modeling
- Study Design
- Survival Analysis
- Target Population
- Time Series
- Type I and Type II Errors
- Unit of Analysis
- Validity
- Volunteer Effect
- Loading...
Get a 30 day FREE TRIAL
-
 Watch videos from a variety of sources bringing classroom topics to life
Watch videos from a variety of sources bringing classroom topics to life -
Read modern, diverse business cases
-
Explore hundreds of books and reference titles

Read next

More like this
Sage Recommends
We found other relevant content for you on other Sage platforms.
Have you created a personal profile? Login or create a profile so that you can save clips, playlists and searches