Entry
Reader's guide
Entries A-Z
Subject index
Mass Casualty Management
When disaster strikes, the greatest imperative is to rescue people, save lives, and treat the injured. The objective of mass-casualty management is to organize logistical facilities, search-and-rescue services, and medical resources in such a way as to minimize loss of life and ensure the complete recovery of as many survivors as possible. Conversely, inefficiency in medical response can result in the loss of lives that could have been saved by more timely and effective intervention.
Disaster epidemiology is the study of the human impact of catastrophe in terms of patterns of death, injury, and disease. Recently, despite considerable increases in population, worldwide disaster mortality has remained fairly constant at about 110,000 persons per year. However, very large variations in the numbers of casualties occur from one disaster to another and with the type of event: for example, the Indian Ocean earthquake and tsunami of December 26, 2004 (magnitude 9.2) killed approximately 297,200 people in 12 countries, which was equivalent to the total natural disaster mortality for the previous five years. Generally, deaths in natural disasters outnumber those in technologically and socially generated disasters by a ratio of 10 to one. Death-to-injury ratios vary considerably: although 1:3 has been hypothesized for earthquakes, 1:6 for floods, and 1:15 for tornadoes, data tend to be poorly recorded and show few stable regularities. In seismic disasters, for example, the ratio of serious to light injuries varies from 1:9 to 1:1,000. Injury typologies are dominated by fractured limbs, cranial trauma, suffocating ingestion of dust, depression of the thorax, and crush syndrome.
Disasters Causing Mass Casualties
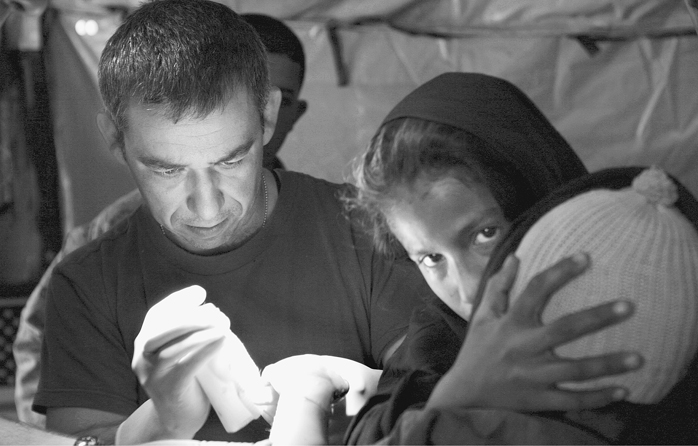
U.S. Navy Commander Joseph Taddeo treats second-degree burns on a 3-year-old Pakistani boy at a field hospital near Shinkiari, Pakistan, after a massive earthquake struck Pakistan, India, and Afghanistan on November 8, 2005. An estimated 80,000 people died
Earthquakes are the archetypical form of sudden-impact disaster that creates a mass-casualty situation, potentially of huge proportions, without warning and in a matter of seconds. Rescue is imperative and, in order to make any impression on the death toll, must occur within 6–12 hours of the main shock, as survival times under rubble are strictly limited by injury, exposure to the elements, and the risk of further structural collapse in aftershocks. Advances in rescue techniques mean that doctors and paramedics are now routinely included in urban search-and-rescue teams. On occasion, medical care is brought to patients even before they are rescued, as medical staff may accompany SAR specialists into the entrapment area.
Whether they are related to volcanism, industrial hazards, terrorism, or other causes, explosions tend to cause some of the most complicated and life-threatening injuries. Primary effects stem directly from the expanding pressure wave and include “blast lung” (pulmonary barotrauma) and compartmental injuries, the result of pressure on internal organs. Secondary injuries are caused by flying objects and shrapnel. Tertiary effects occur when people are flung around by the force of the blast, and quaternary effects can include burns caused by fireballs, and the effects of noxious gases and toxins carried in dust.
Medical Response
When patients are rescued, they should immediately be subjected to triage. This is a form of rationing of medical care as applied to situations in which demand greatly exceeds supply. Primary triage is practiced at the scene of the disaster, or at the advance medical post (first aid post), in order to determine priorities for basic life-support assistance and transportion to a medical center. Secondary triage occurs in the receiving bay of the hospital in order to determine the priorities for clinical and surgical interventions. The basic rationale is to give priority to patients who will benefit the most from some simple form of assistance: victims who are moribund or require major surgery on the basis of an uncertain prognosis are not given high priority.
...
- Africa, North
- Africa, Sub-Saharan
- Asia, East
- Asia, West, Central, and South
- Australia and Pacific Region
- Canada
- Caribbean Island Region
- China
- Desertification
- Earthquake Zones
- Europe, Eastern
- Europe, Western
- Evacuation Routes
- Glacial Melt
- Hurricane Zones
- Japan
- Mediterranean Region
- Mexico
- Middle East
- Ring of Fire
- Russia
- South America
- United Kingdom
- United States, California and West Coast
- United States, Great Lakes
- United States, Hawaii and Pacific Territories
- United States, Mid-Atlantic
- United States, Midwest
- United States, Mountain States
- United States, National
- United States, Northeast
- United States, Northwest and Northern Plains
- United States, Southeast and Gulf Coast
- United States, Southwest
- American Red Cross
- Center for International Disaster Information (CIDI)
- Centers for Disease Control and Prevention (CDC)
- ChildFund International
- Coast Guard, U.S.
- Cooperative for Assistance and Relief Everywhere (CARE)
- Defense, U.S. Department of Direct Relief
- Disaster Preparedness and Emergency Response Associations
- Doctors Without Borders
- Federal Emergency Management Agency (FEMA)
- Food and Agriculture Organization of the United Nations (FAO)
- Habitat for Humanity
- Homeland Security, U.S. Department of Institutional Coordination
- InterAction
- International Law in the Prevention and Mitigation of Disasters
- International Medical Corps
- International Red Cross
- Interpol
- Lutheran World Federation
- Mercy Corps
- National Governments
- Peace Corps
- Red Crescent Society
- Relief International
- Relief Rules
- Salvation Army
- St. Vincent de Paul
- State Governments
- United Nations
- United Nations Children's Fund (UNICEF)
- United Nations Development Programme (UNDP)
- United Nations High Commissioner for Refugees (UNHCR)
- United States Agency for International Development (USAID)
- World Concern
- World Emergency Relief
- World Food Program
- World Health Organization (WHO)
- World Relief
- World Vision
- History of Disaster Relief, Africa
- History of Disaster Relief, Ancient World
- History of Disaster Relief, China and East Asia
- History of Disaster Relief, Europe
- History of Disaster Relief, India
- History of Disaster Relief, Middle East
- History of Disaster Relief, North America
- History of Disaster Relief, Pacific Region
- History of Disaster Relief, Russia
- History of Disaster Relief, South America
- Chemical Disasters
- Cyberattacks
- Economic Disasters
- Food Contamination Disasters
- Gulf Coast Oil Spill (2010)
- Pandemic/Biological Accidents
- Poverty and Disasters
- Radiation Disasters
- Terrorism
- Wars
- Air Transport
- Food Distribution Infrastructure
- Internet
- Mass Transit
- Ports
- Railroads
- Roads
- Schools
- Utilities
- Water Systems
- Community Preparedness
- Community Response
- Evacuation
- Fire Departments
- Home Preparedness
- Local Hazards
- Municipal Offices of Emergency Management
- Personal Preparedness
- Police Departments
- Private Sector Preparedness
- Public Agency Preparedness
- Public-Private Partnerships
- University Preparedness
- Warnings
- Bubonic Plague
- HIV/AIDS
- Malaria (20th Century-Present)
- Measles (1850-Present)
- Severe Acute Respiratory Syndrome (SARS)
- Smallpox (20th Century)
- Tuberculosis (20th Century-Present)
- Earthquakes
- Famine
- Fire
- Floods
- Hurricanes
- Terrorist Attacks
- Tsunami
- Volcanoes
- Wars
- First Aid
- Hysteria
- Pandemic Planning
- Panic
- Panic
- Psychology, Mass
- Psychology, Personal
- Social Work
- Stress Syndromes
- Survivor Guilt
- Working With the Bereaved
- Agricultural Production
- Business Continuity Planning
- Citizen Preparedness Programs
- Cooperation Between Civilian and Military Agencies
- Crisis Management
- Education
- Emergency Response Guidelines and Regulations
- Emergency Rooms
- Evacuation Planning
- Evacuation, Types of
- Exercise Planning
- Food Distribution Systems
- Healthcare
- Hospital Preparedness
- International Standards
- Language Issues and Barriers
- Levels of Nutrition
- Mass Casualty Management
- Media
- National Incident Management System (NIMS)
- National Standards
- Packaging and Tracing of Food
- Paramedics
- Political Economy of Food
- Provision of Food in Disasters
- Refugee Policy
- Refugees, Care of
- Reserve Storage and Transport
- Transportation
- Vulnerable Populations
- Incentives, Intergovernmental and Intersystem
- Mitigation, Benefits and Costs of
- Private Sector, Role in Mitigation
- Public Sector, Role in Mitigation
- Public-Private Interactions in Mitigation
- Regulatory Approaches to Mitigation
- Risk, Government Assumption of
- Risk, Individual Assumption of
- Structural (Engineering) Options for Mitigation
- Avalanches
- Diseases
- Droughts
- Earthquakes
- Fires, Forest
- Fires, Urban
- Floods
- Heat Waves
- Hurricanes/Typhoons
- Landslides
- Pest Invasions
- Sea Surges
- Tornadoes
- Tsunamis
- Volcanoes
- Winter Storms
- Bilateral Versus Multilateral Aid
- Domestic Corruption in International Disasters
- Domestic Politics in International Disasters
- Donations, National
- Donations, Personal
- Funding of International Relief
- Fundraising Cycles
- Politics in International Funding
- Rejection of International Aid
- Intergovernmental Relations and Preparedness
- Planning for Disasters, International
- Planning for Disasters, Local
- Planning for Disasters, National
- Political Support for Preparedness
- Preparedness, Function of
- Preparedness Policy Implementation
- Private Sector, Role in Preparedness
- Research-Based Disaster Planning
- Private Sector, Role in Recovery
- Recovery, International
- Recovery, Local
- Recovery, National
- Recovery, Phases of
- Recovery, Role of Governments in
- Private Sector, Role in Response
- Response, Management Strategies
- Response, Operational Strategies
- Response, Stress Impacts of
- Data Processing
- Early Warning and Prediction Systems
- Funding, U.S.
- Global Warming
- Modeling
- National Oceanic and Atmospheric Administration (NOAA)
- Real-Time Communications
- Research
- Technology
- Technology, Military
- Causes of Complex Emergencies
- Cross-Cultural Interactions
- Cycles of a Disaster
- Disaster Experience
- Education
- Emergency Management Resources
- Ethics of Charity Relief
- Ethnicity and Minority Status Effects on Preparedness
- Gender and Disasters
- Human Rights
- Humanitarian Intervention Versus Humanitarian Action
- Income Inequality and Disaster Relief
- Laws
- Personal Preparedness
- Politics, Domestic
- Politics in International Funding
- Protection of Civilians in Conflict Zones
- Public Policy
- Refugees
- Relief Versus Development
- Risk Communications
- Risk Management
- Risk Perceptions
- Social Impact of Disasters
- Training for Disasters
- Victimology
- United States, California and West Coast
- United States, Great Lakes
- United States, Hawaii and Pacific Territories
- United States, Mid-Atlantic
- United States, Midwest
- United States, Mountain States
- United States, National
- United States, Northeast
- United States, Northwest and Northern Plains
- United States, Southeast and Gulf Coast
- United States, Southwest
- Loading...
Get a 30 day FREE TRIAL
-
 Watch videos from a variety of sources bringing classroom topics to life
Watch videos from a variety of sources bringing classroom topics to life -
Read modern, diverse business cases
-
Explore hundreds of books and reference titles

Read next

More like this
Sage Recommends
We found other relevant content for you on other Sage platforms.
Have you created a personal profile? Login or create a profile so that you can save clips, playlists and searches